I recently read about D-Tree’s case study in Malawi on using mobile-based decision trees for Community Case Management (CCM) at the ict4chw google group mailing list, ICT for Community Health Workers. I was impressed by how organisations like D-Tree are using as simple and ubiquitous a technology as mobiles to better equip health workers.
D-Tree is in the process of creating two mobile phone applications under the ‘Integrated (HIV Effect) Mitigation and Positive Action for Community Transformation’ (IMPACT) project, funded by USAID. The project’s objective is to improve the quality of life of orphans and vulnerable children (OVC) and people living with HIV (PLHIV) in targeted districts of Malawi.
The mobile phone applications that D-Tree is developing are the Child Status Index (CSI) and Community Integrated Management of Childhood Illness (C-IMCI). The tools would help the Health Surveillance Assistants (HSAs) to improve delivery of maternal and child health services, provide supervisory tools to those who manage HSAs and also provide simple logistics management tools to ensure availability of required drugs.
These tools will help increase two-way communications with the communities that were traditionally beyond the periphery of formal health care systems. UNICEF, in a strategic partnership with Frog Design, created a system-level view of how mobile solutions could be used at different levels within the community healthcare system. Before we delve further into the topic, let’s understand what we mean by community case management and health workers.
What is Community Case Management (CCM)?
NGOs and health ministries are increasing their focus on CCM because Community Health Workers (CHWs) are now at the forefront of registering, diagnosing and providing treatment in remote communities, especially to children. Under the CCM strategy, CHWs are trained, supplied with relevant medications and supervised to deliver treatment, primarily to children, for pneumonia, diarrhoea, malaria, new-born sepsis and acute malnutrition.
Community Health Worker: The Last Mile
Often considered as the Last Mile in the supply chain of healthcare, CHWs provide a key role in bridging the access gap to healthcare. These are people from within the community, who are provided training from the clinic, NGOs and/or other government training programs. The CHW is given recognition within the community, is well aware of the health-status within the community and is further motivated to improve its overall health. The CHW works as a liaison between the clinic and the community and also provides basic health knowledge to the community; the CHW is usually rewarded with small incentives.
Bridging the Gap Between Supply and Community Healthcare
Technology alone cannot guarantee progress and solutions to all development problems; it is important to also consider the social, financial and infrastructural needs in increasing impact of the CCM. The Supply Chain Management Subgroup of the CCM Taskforce conducted its first session of the webinar series in May 2013, titled “Overview of the Supply Chain Management for Community Case Management.” The seminar discussed the various challenges and the way forward in supply chain management for CCM. Some of the unique challenges discussed during the webinar included:
- Remote location and tough geography making it difficult to transport medical supplies to communities.
- Limited or challenging transportation networks; limited availability of reliable transport.
- Reliance on community health workers to conduct the work, which is often out of their homes and villages. There is no dedicated physical space.
- Community health workers are at the very end of the supply chain.
- Re-supplies can often take up to 6 months to a year depending on policies and sources. Further delays are possible if the design and essential tools are not in place for dispatching resupplies.
- Additional time for distribution to the CHWs also needs to be considered.
- Proper storage conditions for products are often a challenge, as CHWs work from their homes and in remote places.
According to the seminar, CHWs are reaching some of the most hard-to-reach areas around the world, often with a wide variety of products to manage:
- 30,000 Health Extension Workers (as they are called in Ethiopia) are managing up to 25+ products in Ethiopia;
- 30,000 HSAs in Malawi, with up to 19 products; and
- 35,000+ CHWs in Rwanda are taking care of 5-8 products.
Several factors need to be considered when packaging and supplying products for CCM, as these cannot be the same as those provided in hospitals or other larger health clinics. These factors include – transport and storage conditions (liquids are heavier and more difficult to transport than pills), volume of clients, unique needs of infants and children and the need to make dispensing and manipulating medicines simpler for CHWs (for example, providing pictorial information on the back of a package for easier understanding).
To mitigate issues arising at the re-supply level, CHWs need to be able to estimate needs based on historical data (quantification) – though this can be a challenge if the CHW is new and no prior data exists. In addition, good supply planning is required to ensure there is adequate inventory at all times.
cStock in Malawi, mTrac in Uganda
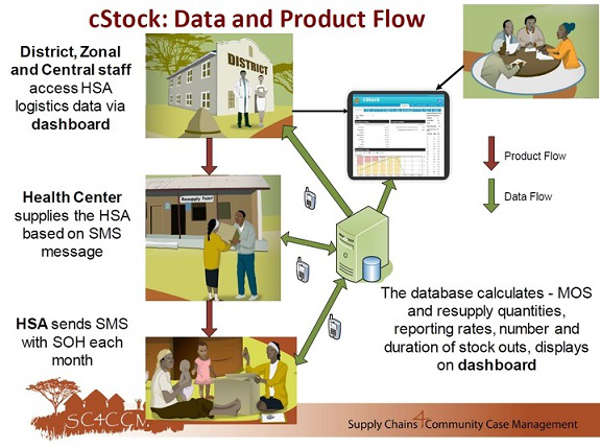
Photo as seen here from Supply Chains4Community Case Management
The Malawi Ministry of Health (MOH), in partnership with a public health research organization, John Snow, Inc. (JSI), has developed a mobile health program called cStock. It is an SMS based reporting and a web-based resupply system. The Health Surveillance Assistants in Malawi use their GSMA mobile phones to report on stock status. Supply chain managers monitor stock levels and stockouts and respond accordingly. The program also sends prompts and reminders to HSAs to file their reports.
Similarly in Uganda, UNICEF in partnership with Ministry of Health and FIND Diagnostics, launched an SMS-based program using RapidSMS to avoid unnecessary stockout of essential medical supplies. It allows health workers to send reports to the District Health teams and National Medical Stores on stock status including information in real-time.
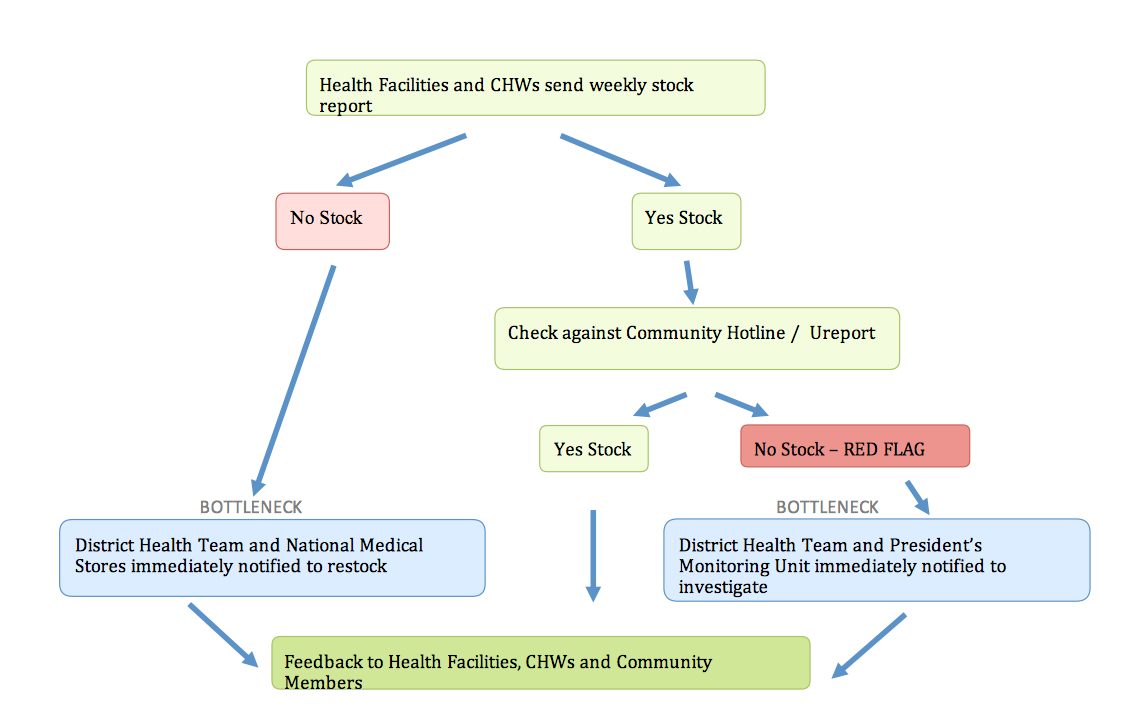
Stock out diagram from mTrac
The program runs in parallel with uReport, where community members can send an SMS to the short code 8200 on Health Service Delivery issues or the on the conduct of health workers. Click here to learn more on how mTrac works.
CHWs are considered to be one of the biggest untapped resources in global healthcare. Using technology and combining efforts to provide actual support and meaning to a CHW’s work has already begun to take shape. And it’s important that those efforts continue.
That’s why many of the features we’re building into engageSPARK focus on increasing engagement not only between organizations and communities, but also between organizations and CHWs. engageSPARK will make it simple for non-tech oriented staff members at NGOs to build SMS and Voice programs that involve interactions among organizations, CHWs, and community members, such as, for example, an NGO enabling a CHW to enrol a pregnant woman into a MAMA pregnancy curriculum.
If you work with CHWs, either as a supervisor or partner, or if you are particularly involved in any of community case management or supply chain management, we encourage you to share your experiences. What are some of the challenges you have faced – especially technology-related issues – and what solutions can you recommend?